Acanthamoeba species
(ah-kan-thah-mee-bah)
Trophozoite
|
Description-
|
|
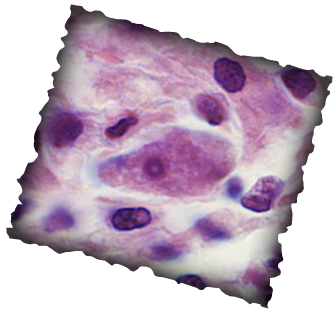
Courtesy of the CDC and Dr. Visvesvara
|
Cyst
|
Description-
|
|
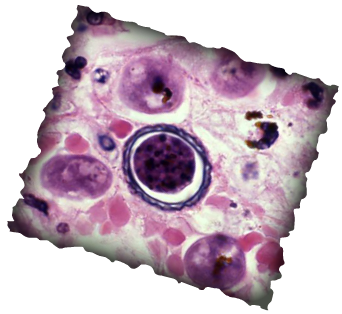
Picture courtesy of the CDC and George Healy, Ph.D.
|
Transmission
This parasite is transmitted to a person by inhalation and aspiration of trophozoites and cysts. It can also be transmitted through the skin or mucosal ulcerations. Once it enters the body, whether through the lungs or the skin, it travels through the bloodstream until the parasite reaches the central nervous system.
Disease
Granulomatous Amebic Encephalitis (GAE)
- Chronic in nature.
- Immunocompromised and the chronically ill are most susceptible.
- Incubation can last weeks to months.
- Symptoms include:
- Headaches, fever, fatigue, stiff neck, altered mental status
- Can cause acanthamoeba keratitis (chronic infection of the cornea).
- People most at risk for this are contact lens wearers and those who have suffered corneal trauma.
- Leads to gradual loss of vision and corneal ulcers.
Diagnostic
- Laboratory specimen
- spinal fluid (trophozoite)
- biopsy of the brain (cyst or trophozoite)
- scrapings from lesions of skin or cornea (cyst or trophozoite)
- Testing
- indirect immunofluorescent staining
- culture on an agar plate, if it has been overlaid with E. coli (bacteria)
- Acanthamoeba spp. feed on the bacteria and will leave visible "tracks" on the agar plate.
- permanent smears made with Giemsa stain or calcofluor white
- Most cases are only diagnosed at autopsy.
Treatment
- Treatment with sulfamethazine is suggested, if the parasite is identified in time (before death).
- Amebic keratitis treatment includes
- ketoconazole
- miconazole
- propamidine
- pentamidine
- rifampin
- The sooner the treatment, the better the prognosis.
